INTRODUCTION
For the success of endodontic treatment, it is essential that there be a significant reduction of the pathogens present in the root canal system, therefore, the chemical - mechanical preparation of it is the fundamental pillar that will lead to the success or failure of the treatment, Machado et al., 20151. However, even after such preparation, bacteria can persist within the root canals, so some authors recommend the use of intra-duct medication between sessions2. Calcium hydroxide being the most widely used medicine for its antibacterial and biocompatibility properties. After its application, intra-duct medication must be removed in order to condition the dentinal surface and promote the ideal physical and chemical conditions to achieve optimal sealing, since its retention in the dentin walls negatively influences the characteristics of the sealing cements2-5. Thus, the complete and predictable removal of the Ca (OH)2 dressing before filling the root canal is critical and could be directly related to the endodontic treatment outcome6.
Additionally, the penetration of the sealant in the dentinal tubules is essential to improve the adaptation and retention of the sealant cement and act as a physical barrier in the irregularities, dentinal tubules and lateral channels avoiding the entry of microorganisms into the dentinal tubules7,8. Ah plus sealant cement (Dentsply Maillefer, Ballaigues, Switzerland) has excellent physicochemical properties that have been widely studied, which is why it is considered a gold standard to evaluate new cements9-11. The remnants of calcium hydroxide used as intracanal medication could result in a variation of physical and chemical properties such as particle size, solubility, viscosity and surface tension, which could influence the amount of penetration depth9.
In the evaluation of the degree of penetration of substances into the dentinal tubules, confocal laser scanning microscopy (CLSM) has been frequently used allowing detailed information on the level of insertion of pastes and cements in the dentinal tubules10. In this way, CLSM could be used to assess the degree of penetration of Ca (OH)2 and sealing cements in dentinal tubules and how much of this material remains after the use of removal techniques. For the above, the following null hypothesis was raised: Intraduct medication with calcium hydroxide paste does not decrease the penetration of the sealing cement in the dentinal tubules.
Materials and methods
Twenty palatine roots of upper molars were cut, standardized in 12 mm and explored with a file type K # 10 (Dentsply Maillefer). Immediately afterwards they were instrumented at 11mm with a manual file type K # 15 and 20 (Dentsply Maillefer,); subsequently they were instrumented with the Wave One Large System (Dentsply Maillefer) by means of three pecking movements until they reached the working length. During instrumentation the root canal was irrigated with 5ml of 5.25% NaOCl between each instrument. Finally, the final irrigation was performed with 10 ml of 5.25% sodium hypochlorite activated with an ultrasonic insert (IRRI S, VDW, Munich), for 2 activation cycles of 30 seconds followed by 5ml EDTA at 17% ( MD.Cleanser Meta Biomed Chungcheongbuk-do, Korea) for 3 minutes and finally 10ml of distilled water. Subsequently, they were dried with Wave One golde medium (Dentsply Maillefer) paper cones.
The samples were paste with heavy silicone (Speedex Putty, Coltene, Switzerland) in plates of cell culture wells (Falcon VWR, Spain) leaving empty wells to later be filled with water to maintain a humid environment. Subsequently, the roots were randomly distributed in 2 groups (n = 10 per group):
- Group 1 (Ah Plus + Rhodamine B 0.01%) .- Immediately after instrumentation the channels were sealed with the single cone technique. For this, the resin resin sealer of root canal Ah plus (Dentsply Maillefer) was mixed in a proportion 1; 1 with a small amount of rhodamine-B (0.1%) (Sigma Aldrich, Darmstadt, Germany), up to that the mixture became uniform fuchsia color. Subsequently, the cement was taken inside the canal with a Wave one large gutta-percha cone (Dentsply Maillefer) brushing the walls of the cervical third, middle and finally taken to working length. The cut at the entrance of the duct with a hot instrument (Gutta cut, Surident Mart, Arumbakkam, Chennai) followed by vertical compaction with a metal trainer compatible with the diameter of the channel mouth. Finally, we proceeded to clean the surface of the entrance to the duct with a cotton ball soaked with 70 ° alcohol and seal the entrance of the canal with temporary cement.
- Group 2 (Ca (OH) 2 / Ah Plus + Rhodamine B 0.01%).- Immediately after instrumentation, a calcium hydroxide paste (Eufar, Bogotá, Colombia) with propylene glycol was placed inside the root canal powder (0.25 g / 0.1ml) using a # 35 spiral lentulum (Dentsply Maillefer) and subsequent compaction with one and compacting it with a # 3 plugger (Dentsply Maillefer). Then, the samples were stored at 37 ° C with 100% humidity for 15 days (Fanem São Paulo - SP, Brazil). After that period, the paste was removed from the inside of the canal with the recapitulation technique using a Wave One Large file (Dentsply Maillefer). Subsequently, the channels were irrigated with 15 ml of 5.25% sodium hypochlorite, followed by 5ml EDTA at 17% (MD.Cleanser Meta Biomed Chungcheongbuk-do, Korea) for 3 minutes and 10 ml of distilled water. Finally, the channels were sealed with the single cone technique with Ah plus cement (Dentsply Maillefer) mixed rhodamine-B (0.1%) (Sigma Aldrich) following the same procedures described for group G1.
After the sealing procedures, both groups were stored at 37 ° C 100% humidity for a minimum of 7 days (Fanem São Paulo - SP, Brazil). Subsequently, the roots were cut into three sections with a precision metallographic closure (IsoMet 1000 Buehler, Illinois) from apical to 3 mm, 6 mm, 9 mm, corresponding to the apical, middle and cervical thirds. Once divided, each section was polished in a double polisher variable speed (Ecomet - Politriz, Buehler, Illinois). Subsequently, each section was observed through confocal laser scanning microscopy (Leica, Mannheim, Germany) at a 4X magnification by scanning at 10 µm surface depth and using an absorption wavelength of 540 nm and of emission of 590 nm, corresponding to the wavelength of rhodamine-B. The obtained photomicrographs were analyzed in the Image J program to determine the maximum penetration (figure 1) of the cement inside the dentinal tubules.
The obtained data were tabulated for statistical analysis through the ANOVA test followed by Tukey's post hoc test for intra-group analysis; and of teste T for independent data for intergroup analysis. The level of significance used for these tests was p <0.01.
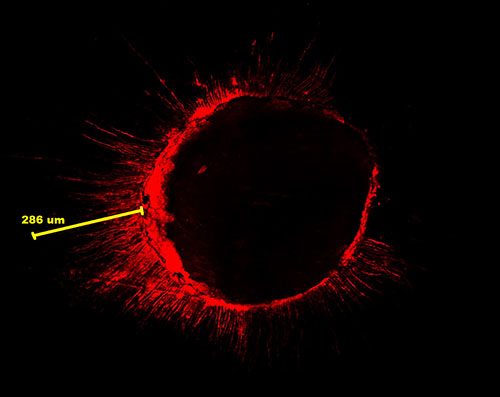
Figure 1. Maximum penetration of the sealing cement inside the dentinal tubules
Results
The penetration of cement Ah plus inside the dentinal tubules in all thirds of the root canal analyzed was significantly lower in the group where intracanal medication with the paste based on calcium hydroxide was used prior to filling (p <0.01 ) (table 1, figure 1).
In the group sealed with Ah plus cement without prior placement of calcium hydroxide before the filling was observed that the penetration of the cement in the tubules was significantly lower in the apical third, followed by the middle and finally by the cervical (p <0.01 ). In the group sealed with Ah plus cement with previous placement of calcium hydroxide before filling it was observed that the penetration of the cement in the tubules was significantly lower in the apical third (p <0.01) and without significant difference between the middle third and cervical (p> 0.01) (table 1, figure
Tabla 1. Maximum penetration (µm) of Ah plus cement inside the dentinal tubules after using or not using intracanal medication based on calcium hydroxide
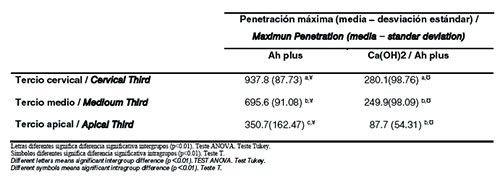
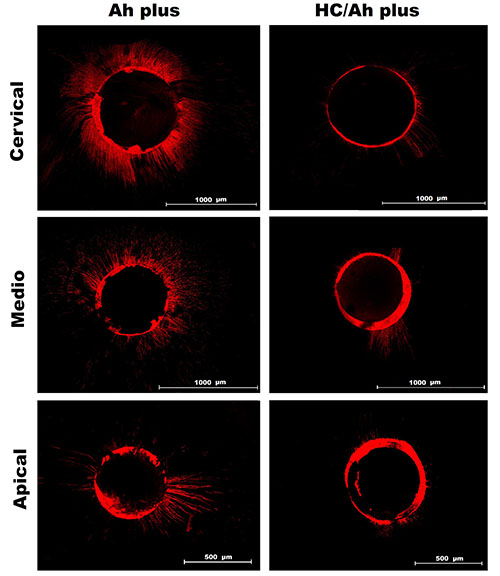
Figure 2. Photomicrographs of the channels sealed with Ah plus cement without and with previous placement of calcium hydroxide (HC) as intra-channel medication.
Discussion
To achieve maximum effectiveness, it is important that the paste homogeneously fill the root canal throughout its entire length of work12, to fulfill this purpose in this study, the calcium hydroxide paste was placed with a lentulum, a method considered as the most effective for the insertion of paste into the root canal system13-17. However, during endodontic filling procedures, calcium hydroxide remnants can act as a barrier and prevent penetration of sealant cement into dentinal tubules4, despite advances in technology, no technique completely removes the dressing of Ca (OH)22,18-23. Due to the difficulties in removing the medication with Ca (OH)2 paste, the remnants could act as a dentin bar (chemical layer) and cause difficulties in the penetration of the sealing cement, which would contribute to apical microfiltration. In the present study it was shown that calcium hydroxide decreases the depth of penetration of cement into dentinal tubules (p <0.01).
These findings agree with the research of Uzunoglu et al. 201824, who conducted an investigation on the effect of calcium hydroxide on the penetration of dentinal tubules in a sealant based on epoxy resin (AH-26) and tricalcium silicate (BioRoot RCS), premolars were used in which depth of penetration was analyzed using a confocal laser microscope, showing that the remains of the calcium hydroxide medication significantly decreased the depth and the percentage of penetration in the dentinal tubules with the AH-26 and BioRoot sealant in the three thirds. The effect of residual calcium hydroxide on cement penetration could be related to the interaction of its physicochemical properties such as; Composition, pH film thickness, wettability, and flow25.
However, the results of the current investigation differs from that published by Cruz et al. 201726, in which, they conducted a study with the purpose of evaluating the effect of calcium hydroxide (HC), on the tubular penetration of two endodontic sealants, Ah Plus and MTA Fillapex, identifying that the use of Intracanal CH did not interfere with sealant penetration in the apical third of the canal; however, the penetration of Ah Plus in the middle third decreased.These results can be caused by different parameters such as the root canal anatomy, the size and density of the dentinal tubules, the difficulty in completing the elimination of the intracanal HC medication and the dentinal slit21,22. Bernardes et al. 201027, reported that with or without the presence of HC residues, sealability penetrability tends to increase in the aponal-coronal direction; These results are consistent with those of the current investigation.
Akcay et al. 201628, argue that the depth of penetration in the dentinal tubules of five sealing cements and the third of the root with greater penetration thereof, by confocal laser microscopy, the third of the root canal that presented greater cement penetration sealant was the coronal third followed by the middle third and finally the apical third that presented a smaller area of penetration of the sealant cement; results that coincide with those of this study in terms of penetration, because the cervical third was the one with the greatest depth and percentage penetration followed by the middle third and finally the apical third of the root canal. In addition, the sealing cement AH presented a low penetration in the dentinal tubules in the apical third in both groups probably because the apical third frequently presents obliteration of the dentinal tubules.
Many factors could have an effect on the penetration of materials into the dentinal tubules, such as the smear layer29, the physical and chemical properties of the materials30 and the anatomy of the tooth13, the characteristics of the Dentin surface can also affect the penetration of root canal sealants31.
Chandra et al. 201232, mention that previously the investigations to evaluate the penetration of sealing cements inside dentinal tubules were carried out with a light microscope, with the years they continued advancing and the scanning electron microscope was used. However, due to its disadvantages such as: the difficulty of distinguishing dentin cement from the root canal; the presence of artifacts in the final image and the greater time invested in observation33, the confocal laser microscope has been used more frequently in recent years for its several advantages: high vertical and horizontal resolution allowing a three-dimensional study of the samples, ability to control depth of field and collect optical sections, ability to differentiate different structures dyed with fluorophores with greater contrast, possibility of performing a 3D reconstruction of the digitized images obtained from each sample, which can be analyzed with different software. The confocal laser microscope uses a laser source to promote the excitation of fluorophores. Lasers can diffuse through dentin, enamel and biofilms, thus detecting their internal structures and forming several images.
This technology provides reliable information on the distribution of CH and sealing cements along the circumference of the root canal wall. Tedesco et al. 201834, compared the measurement accuracy with confocal laser microscope with scanning electron microscope. They evaluated the penetration inside the dentinal tubules of two sealing cements compared Endofill and Ah Plus. As a result, they obtained that penetration inside the dentinal tubules showed a significant difference between the observation methods for the two sealing cements, that is, in the samples analyzed with confocal laser microscopy, a greater amount of tubules was observed dentiners with cement sealant inside and greater depth of penetration of cement.
Conclusions
Intra-channel medication with Ca (OH) 2 after filling the root canal decreases the penetration depth of the sealing cement Ah plus in the dentinal tubules. Penetration of sealants in dentinal tubules increases in the coronal apical direction.
Conflict of interests
The authors declare that they have no conflicts of interest.
Bibliografía
- De Lima Machado ME. Endodoncia: ciencia y tecnología. México: AMOLCA; 2016.
- Hosoya N, Kurayama H, Lino F, Arai T. Effects of calcium hydroxide on physical and sealing properties of canal sealers. Int Endod J. 2004 Mar; 37(3): p. 178-84.
- Nandini S, Velmurugan N, Kandaswamy D. Removal efficiency of calcium hydroxide intracanal medicament with two calcium chelators: volumetric analysis using spiral CT, an in vitro study. J Endod. 2006 Nov; 32(11): p. 1097-101.
- Böttcher D, Hirai V, Da Silva Neto U, Grecca F. Effect of calcium hydroxide dressing on the long-term sealing ability of two different endodontic sealers: an in vitro study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 110(3): p. 386-9.
- Kok D, Rosa R, Barreto M, Busanello F, Santini M, Pereira J. Penetrability of AH plus and MTA llapex after endodontic treatment and retreatment: a confocal laser scanning microscopy study. Microsc Res Tech. 2014 Jun; 77(6): p. 467-71.
- Zorzin J, Wießner J, Wießner T, Lohbauer U, Petschelt A, Ebert J. Removal of Radioactively Marked Calcium Hydroxide from the Root Canal: Influence of Volume of Irrigation and Activation. J Endod. 2016 Apr; 42(4): p. 637-40.
- Camargo E, Vivan R, Bramante C, Duarte M, Graeff M, Silva P, et al. The influence of calcium hydroxide on adaptation and root canal penetration in teeth filled with methacrylate-based resin sealer. Dental Press Endod. 2015 Sept-Dec; 5(3): p. 21-7.
- Kim S, Kim Y. Influence of calcium hydroxide intracanal medication on apical seal. Int Endod J. 2002 Jul; 35(7): p. 623-8.
- Mamootil K, Messer H. Penetration of dentinal tubules by endodontic sealer cements in extracted teeth and in vivo. Int Endod J. 2007 Nov; 40(11): p. 873-81.
- Deniz Sungur D, Aksel H, Purali N. Effect of a Low Surface Tension Vehicle on the Dentinal Tubule Penetration of Calcium Hydroxide and Triple Antibiotic Paste. J Endod. 2017 Mar; 43(3): p. 452-455.
- Viapiana R, Moinzadeh A, Camilleri L, Wesselink P, Tanomaru Filho M, Camilleri J. Porosity and sealing ability of root fill- ings with gutta-percha and BioRoot RCS or AH Plus sealers. Int Endod J. 2016 Aug; 49(8): p. 774-82.
- Zavala L. Efecto inhibidor de la clorhexidina gel al 2 % y del hidróxido de calcio mezclados con tres diferentes vehículos (solución de clorhexidina al 2 %, paramonoclorofenol alcanforado y suero fisiológico) ante la presencia de Enterococcus faecalis. Lima: Universidad Wiener; 2014.
- Estrela C, Mamede Neto I, Lopes H, Estrela C, Pécora J. Root canal filling with calcium hydroxide using different techniques. Braz Dent J. 2002; 13(1): p. 53-6.
- Chybowski E, Glickman G, Patel Y, Fleury A, Solomon E, He J. Clinical Outcome of Non-Surgical Root Canal Treatment Using a Single-cone Technique with Endosequence Bioceramic Sealer. J Endod. 2018 Jun; 44(6): p. 941-945.
- Monticelli F, Sword J, Martin R, Schuster G, Weller R, Ferrari M, et al. Sealing properties of two contemporary single-cone obturation systems. Int Endod J. 2007 May; 40(5): p. 374-85.
- Faga E, Gonzales L, Taccio G, Dos Santos M, Antoniazzi J, Gavini G. Presence of Voids after Continuous Wave of Condensation and Single-cone Obturation in Mandibular Molars: A Micro-Computed Tomography Analysis. J Endod. 2017; 43(4): p. 638-642.
- Ho C, Khoo A, Tan R, Teh J, Lim K, Sae L. pH changes in root dentin after intracanal placement of improved calcium hydroxide containing gutta-percha points. J Endod. 2003 Enero; 29(1): p. 4-8.
- Capar I, Ozcan E, Arslan H, Ertas H, Aydinbelge H. Effect of different irrigation methods on the removal of calcium hydroxide from an artificial standardized groove in the apical third of root canals. J Endod. 2014 Mar; 40(3): p. 451-4.
- Pompermayer A, Abreu R, Favarin M, Wagner M, Vinícius M, Kuga M, et al. The effect of final irrigation on the penetrability of an epoxy resin-based sealer into dentinal tubules: a confocal microscopy study. Clinical Oral Invest. 2015; 13(9): p. 233-239.
- Kara T. Effect of QMix 2in1 on Sealer Penetration into the Dentinal Tubules. J Endod. 2015 Febrero; 41(2): p. 257-260.
- Yaylali I, Kececi A, Kaya B. Ultrasonically activated irrigation to remove calcium hydroxide from apical third of human root canal system: a systematic review of in vitro studies. J Endod. 2015 Octubre; 41(10): p. 1589–1599.
- Castagna F, Rizzon P, Rosa R, Santini M, Barreto M, Duarte M, et al. Effect of passive ultrassonic instrumentation as a final irrigation protocol on debris and smear layer removal–a SEM analysis. Microsc Res Tech. 2013 Mayo; 76(5): p. 496-502.
- Gupta R, Sharma H, Kumari R, Prakash N, Rai N, Jain R. Effectiveness of two techniques in removal of calcium hydroxide medicament from root canals: An in vitro assessment. Journal of Clinical and Diagnostic Research. 2018 Septiembre; 12(7): p. 309-312.
- Uzunoglu E, Erdogan O, Aktemur S. Effect of calcium hydroxide dressing on the dentinal tubule penetration of 2 different root canal sealers: a confocal laser scanning microscopic study. J Endod. 2018 Junio; 44(6): p. 1-6.
- Rodríguez G, Álvarez M, García J. El hidróxido de calcio: su uso clínico en la endodoncia actual. AMC. 2005 mayo-junio; 9(3): p. 143-152.
- Cruz A, Grecca F, Piaseckii L, Wichnieski C, Westphalen V, Carneiro E, et al. Influence of the calcium hydroxide intracanal dressing on dentinal tubule penetration of two root canal sealers. European Endodontic Journal. 2017 Junio; 2(1): p. 3-6.
- Bernardes R, De Amorim C, Junior D, Pereira L, Duarte M, Moraes I, et al. Evaluation of the flow rate of 3 endodontic sealers: sealer 26, AH plus and MTA obtura. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Enero; 109(1): p. 47-49.
- Akcay M, Arslan H, Durmus N, Mese M, Capar I. Dentinal Tubule Penetration of AH Plus, iRoot SP, MTA Fillapex, and GuttaFlow Bioseal Root Canal Sealers After Different Final Irrigation Procedures: A Confocal Microscopic Study. Lasers Surg Med. 2016 Jan; 48(1): p. 70-6.
- Hülsmann M, Ove , Peters , Dummer P. Mechanical preparation of root canals: shaping goals, techniques and means. Endodontic Topics. 2005; 10(1): p. 30–76.
- Flores D, Rached F, Versiani M, Guedes D, Sousa-Neto M, Pécora J. Evaluation of physicochemical properties of four root canal sealers. Int Endod J. 2011 Feb; 44(2): p. 126-35.
- Adl A, Hamedi S, Sedigh Shams M, Motamedifar M, Sobhnamayan F. The ability of triple antibiotic paste and calcium hydroxide in disinfection of dentinal tubules. Iran Endod J. 2014 Mar; 9(2): p. 123-6.
- Chandra S, Shankar P, Indira R. Depth of Penetration of Four Resin Sealers into Radicular Dentinal Tubules: A Confocal Microscopic Study. J Endod. 2012 Abr; 38(10): p. 1412-1416.
- Van Meerbeek B, Vargas M, Inoue S, Yoshida Y, Perdigão J, Lambrechts P, et al. Microscopy investigations. Techniques, results, limitations. Am J Dent. 2000 noviembre; 13(Spec No): p. 3-18.
- Tedesco M, Carvalho M, Antunes E, Fonseca L, Hecke A, Silveira C. Comparison of two observational methods, scanning electron and confocal laser scanning microscopies, in the adhesive interface analysis of enxdodontic sealers to root dentine. Clinical Oral Investigations. 2018; 22(1): p. 2353–2361.
 |
Virginia, Veintimilla; https://orcid.org/0000-0003-0850-1531 |
| Raquel, Guillen; https://orcid.org/0000-0002-4177-1499 |
| Héctor, Caballero; https://orcid.org/0000-0001-5479-8263 |
| Manoel, Machado; https://orcid.org/0000-0001-7899-4576 |

Reconocimiento-NoComercial-CompartirIgual
CC BY-NC-SA
Esta licencia permite a otros entremezclar, ajustar y construir a partir de su obra con fines no comerciales, siempre y cuando le reconozcan la autorÍa y sus nuevas creaciones estÉn bajo una licencia con los mismos tÉrminos.