RESUMEN
La corticotomía se define como una osteotomía, en la cual, se corta el hueso cortical, perforando o alterando mecánicamente de una manera quirúrgica controlada y al mismo tiempo penetrando mínimamente en la médula ósea para acelerar el movimiento dental ortodóntico en respuesta a una demanda de los pacientes en cuanto a la efectividad del tratamiento y al rápido movimiento de cada zona. Objetivo: Mediante una revisión bibliográfica, determinar la distancia y tiempo en que se logra llevar a cabo un desplazamiento o movimiento ortodóntico después de haber realizado una corticotomía selectiva. Para la búsqueda, se utilizaron plataformas como Pubmed, Scielo, Science Direct y Google Scholar, en las que se empleó palabras claves como distancia, tiempo, corticotomía selectiva y tratamiento de ortodoncia y se buscaron artículos publicados entre el 2001 y 2017. Resultados: se obtuvo que los movimientos se realizan en un periodo de 4 meses, respecto a la distancia y se observó que se logra desplazar un promedio de 3.5 mm. Conclusiones: En pacientes adultos, ha aumentado la exigencia sobre reducir tiempos de tratamiento, la ortodoncia facilitada por corticotomía consigue llevar a cabo un tratamiento exitoso y disminuir los tiempos de tratamiento. Sin embargo, la evidencia es escasa, pues está basada principalmente en reportes de casos, por lo cual se requiere mayor investigación acerca de este procedimiento.
Palabras clave: Ortodoncia; osteotomía; hueso cortical; remodelación ósea; tiempo de tratamiento..
ABSTRACT
Corticotomy is defined as an osteotomy, in which the cortical bone is cut, perforated or mechanically altered in a controlled surgical way and at the same time minimally penetrating the bone marrow to accelerate orthodontic dental movement in response to a demand for patients regarding the effectiveness of the treatment and the rapid movement of each zone. Objective: by means of a bibliographic review, determine the distance and time in which an orthodontic movement is achieved after having performed a selective corticotomy. For the search, Platforms such as Pubmed, Scielo, Science Direct and Google Scholar were used, in which keywords such as distance, time, selective corticotomy and orthodontic treatment were used and articles published between 2001 and 2017 were searched. Results: It was obtained that the movements are carried out in a period of 4 months, with respect to the distance and it was observed that an average of 3.5 mm can be moved. Conclusions: in adult patients, the demand for reducing treatment times has increased; orthodontics facilitated by corticotomy achieves successful treatment and decreases treatment times. However, the evidence is scarce, since it is mainly based on case reports, so more research is required about this procedure.
Keywords: Orthodontics; osteotomy; cortical bone; bone remodeling; treatment time.
RESUMO
A corticotomia é definida como uma osteotomia, na qual o osso cortical é cortado, perfurado ou alterado mecanicamente de maneira cirúrgica controlada mais penetração mínima na medula óssea para acelerar o movimento dentário ortodôntico em resposta a uma demanda por pacientes quanto à eficiência do tratamento e ao movimento rápido de cada zona. Objetivo: por meio de uma revisão bibliográfica, determinar a distância e o tempo em que um movimento ou deslocamento ortodôntico é alcançado após a realização de uma corticotomia seletiva. Material y métodos: Para a pesquisa, foram utilizadas plataformas como Pubmed, Scielo, Science Direct e Google Scholar, nas quais foram utilizadas palavras-chave como distância, tempo, corticotomia seletiva e tratamento ortodôntico e foram pesquisados artigos publicados entre 2001 e 2017. Resultados: se observou que os movimentos são realizados em um período de 4 meses, em relação à distância observou-se que uma média de 3,5 mm pode ser movimentada. Conclusões: em pacientes adultos, a demanda por redução do tempo de tratamento aumentou, a ortodontia facilitada pela corticotomia consegue o sucesso do tratamento e diminui o tempo de tratamento. No entanto, as evidências são escassas, uma vez que se baseiam principalmente em relatos de casos, sendo necessárias mais pesquisas sobre esse procedimento.
Palavras-chave: Ortodontia; osteotomia; osso cortical; remodelação óssea; tempo de tratamento.
INTRODUCTION
The orthodontics facilitated by corticotomy corresponds to a modern surgical technique described for the first time by Heinrich Köle, in 19591. Until now, it was thought that the accelerated dental movement was due to the displacement of the bone segment individually, but in 2001 Wilcko et al2 demonstrate that the speed of dental movement is due to a local and transient demineralization / remineralization in the alveolar bone compatible with the accelerated regional phenomenon (RAP)3,4.
Corticotomy is defined as osteotomy of the cortical bone. It is a procedure by which only cortical bone is cut, perforating or mechanically altering, in a controlled surgical way and at the same time minimally penetrating the bone marrow1,2. H. Frost describes the so-called regional acceleration phenomenon (rap) as a physiological process that is observed after an aggression in hard and / or soft tissues and consists of an acceleration of the healing process with a greater bone cell turnover and a decrease in regional bone densities4.
Orthodontics in general has evolved in terms of techniques and mechanics that have helped to generate changes when establishing the treatment plan5. Within the advantages of corticotomy we have that it serves to accelerate the movement of the teeth, the bone can be increased, thus avoiding periodontal defects that occur as a result of a thin alveolar bone. Despite being a convenient auxiliary technique, we can find disadvantages such as being considered an invasive procedure, the risk of damage to adjacent vital structures, postoperative pain, inflammation, chances of infection, and avascular necrosis5,6.
The bad dental position is responsible for aesthetic and occlusal problems in many adults, this can be caused by severe factors that include an advanced periodontal problem, dental migration due to tooth loss and dental movements caused by occlusal trauma7. The clinical indications for the use of corticotomy have been wide, reporting success in the management of surgically assisted palatal expansion, bimaxillary dentoalveolar protrusion, anterior open bite, severe skeletal protrusion and dental crowding, additionally they are used in adult patients to accelerate the time of orthodontic treatment8.
The demand of the patients regarding the effectiveness of the treatment is increasingly acceptable since they refer to a great change both in their oral structure and in the rapid movement of each of the area in which it was performed in either specific or generalized treatment8,9. This is why this article aims to present results of a bibliographic review, determine the distance and time in which an orthodontic movement or displacement is achieved after having performed a selective corticotomy.
Materials and methods
The information was obtained through the bibliographic review of articles in digital format, published from 2001 to 2017. Platforms such as Pubmed, Scielo, Science Direct and Google Scholar were used, in which keywords such as selective corticotomy, distance, rap were used , orthodontics, alveolar bone, dental movement. For the selection, the importance of its scientific value and updating was raised as an inclusion criterion. As exclusion criteria, articles published more than 17 years ago were discarded. 65 articles were reviewed and a selection of 33 was made, complying with the inclusion criteria already mentioned.
Results
The objective of this study was to conduct a bibliographic review of the distance and time of movements with selective corticotomy in orthodontic treatments. Of the 33 articles that were analyzed, it was found that there is an average of 4 months in which the dental movement is performed, the time that the bone has while it is remineralized again9,10,11,12,13,14,15.
On the other hand, in terms of the distance of displacement it was found that movements such as mesialization, distalization, intrusion and extrusion, are commonly used by the corticotomy method, and that progress is made approximately 3.5 mm thus reducing 50% of the treatment period16,17,18,109,20,21,22.
It was observed that experimental studies in animals report as a consequence of corticotomy an increase in the speed of dental movement, with average movement rates in the corticotomy group of 4.67 ± 0.58 mm. 2.33 ± 0.58 mm in the control group16,17,18,109,20,21,22.
In addition, some case reports in humans with corticotomy, show that the treatment time ranges between 4 and 18 months depending on the complexity of the malocclusion9,10,11,12,13,14,15,3,16,17,18,109,20,21,22.
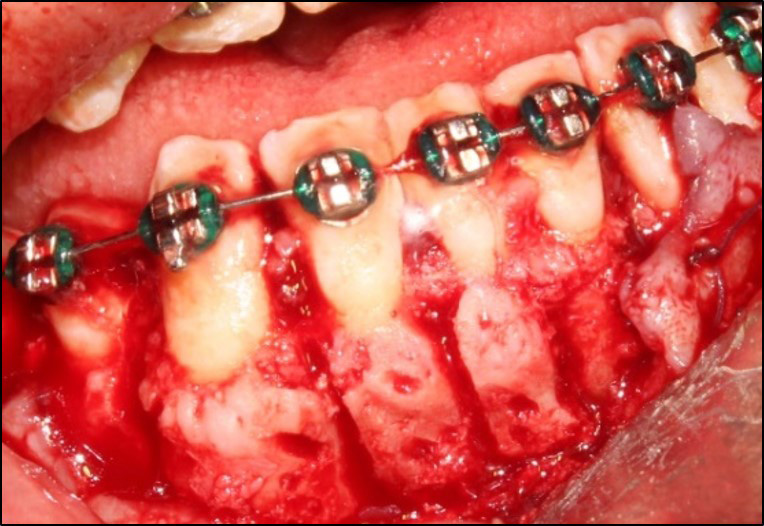
Figure 1. Selective corticotomy, courtesy of the C.D. Querly Cuellar.
Discussion
Selective corticotomy was first introduced by Heinrich Köle, in 1959, who developed a technique that consists of cutting cortical bone into blocks, leaving the entire mobile segment, this technique was little accepted because it was very invasive. However, in 2001, the Wilcko brothers modified this technique and developed a protocol that consists of making cuts in the cortical bone through the use of a round surgical drill, without drilling or leaving it mobile, and after that applying bone grafting. This proposed technique, unlike Köle's, was very well accepted and is currently used3,16,24.25.
The speed of tooth movement is an important factor that determines the duration of orthodontic treatment. Physiologically, the speed of movement of the teeth reflects the rates of bone turnover and remodeling. Previous approaches by authors such as Yamasaki17, mention that corticotomy has been used in an attempt to accelerate the movement of teeth, with this approach techniques such as low energy laser irradiation, magnetic fields, pharmacological interventions with injection have also been included of prostaglandin E2 17 and vitamin D26,27,28,29.
Selective corticotomies are considered a useful tool in orthodontics, since they allow working in malocclusions such as biprotrusions; according to Frost 30 (2006), in just 1 year of treatment, he was able to successfully complete a case of 4 extractions, with a slight orthodontic force of 1 N (Newton). It is well known that a 4.5 N force is generally used for conventional orthodontic treatment, so that movement can be performed, however, in this case, thanks to the alveolar corticotomy, a smaller force could be implemented, and by less time. Total orthodontic treatment was dramatically reduced from 31 months, which is an average treatment period for cases with extractions, to 12 months, having a total reduction of 50% of the time31,32.
Akay and cols.10 conclude that on average a molar, with a previous corticotomy, can be intruded from 3.1 to 3.5 mm in just 12 to 15 weeks of intrusion period with forces of 200 to 300 g. This finding supports the view that combining corticotomy with orthodontic biomechanics has the potential to shorten the period of time33.
T. Motohashi27, showed in his article that the greatest displacement was achieved in cases combined with corticotomy, suggesting that not only the teeth, but also the anterior alveolar segment is moved in block by an orthodontic treatment combined with corticotomy34. This statement corroborates the studies presented by Wang and cols. Pavlin, 2001, reported as a consequence of corticotomy an increase in the speed of dental movement, with average movement rates in the corticotomy group of 4.67 ± 0.58 mm. 2.33 ± 0.58 mm in the control group34.
In relation to time, the studies carried out by Wilcko and cols., 2009; coincide with the research of Akay and cols., 2009, which shows that the treatment time ranges between 4 and 18 months according to the complexity of the malocclusion. The above suggests that corticotomy may be a viable alternative in some patients3,10,16.
Conclusions
Currently, the demand for reducing orthodontic treatment times has increased; the orthodontics facilitated by corticotomy is able to carry out a successful treatment, reducing times considerably. However, the evidence is scarce, since it is mainly based on case reports, so more research is required about this procedure.
Interest Conflict
The authors declare no conflict of interest in the presentation of data, preparation and publication of this article.
Bibliografía
- Bhattacharya P. Assessment of corticotomy facilitated tooth movement and changes in alveolar bone thickness - A CT Scan study. Journal of Clinical and Diagnostic Research. 2014 Octubre; 8(10).
- Murphy H. Periodontal Accelerated osteogenic orthodontics: a description of the surgical technique. J Oral maxillofac surg. 2009; 67(21).
- Wilcko WM WTBJFD. Rapid orthodontics with alveolar reshaping: two case reports of decrowding. Int J periodont Restorat Dent. 2001; 21(1).
- Burrow. S. Biomechanics and the paradigm shift in orthodontic treatment plannin. J Clin Orthod. 2009; 43(10).
- Dibart S S. Piezocision: a minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Practical Osseous Surgery in Periodontics and Implant Dentistry. 2011;(195).
- Dibart S S. Piezocision: a minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Practical Osseous Surgery in Periodontics and Implant Dentistry. 2011;(195).
- Nowzari YH. Periodontally accelerated osteogenic orthodontics combined with autogenous bone. Compend contin Educ Dent. 2008; 29.
- Samuel Salvador Robles Andrade CGCCHH. Ortodoncia acelerada periodontalmente: Fundamentos biológicos y técnicas quirúrgicas. Revista Mexicana de Periodontología. 2011 abril; 2(1).
- Arango JDCMR. Comparación Clínica entre el tratatmiento ortódontico facilitado por corticotomia y ortodoncia convencional. Int. J odontostomat. 2015; 9(2).
- Akay M AAGTASKB. Enhanced effect of combined treatment with corticotomy and skeletal anchorage in open bite correction. J Oral Maxillofac Surg. 2009;(67).
- Dubravko Pavlin DMD MPD,RAMVRDMPTGDPD. Cyclic Loading (Vibration) Accelerates Tooth Movement in Orthodontic Patients: A Double-Blind, Randomized Controlled Trial, Semin Orthod. http://dx.doi.org/10.1053/j.sodo.2015.06.005.
- Düker I. experimental animal research into segmental alveolar movement after corticotomy. J Maxillofac Surg. 1975; 3.
- Shoichiro L SSGITNTISM. Acceleration of orthodontic tooth movement by alveolar corticotomy in the dog. Am J Orthod Dentofacial Orthop. 2007; 131(4).
- L Soichiro SSMS. An adult bimaxillary protrusion treated with corticotomy-facilitated orthodontics and titanium miniplates. Angle orthodontist. 2006; 76(6).
- Sumit Yadav aTDAAHGZKaRNFC. Effect of low-frequency mechanical vibration on orthodontic tooth movement.. Am J Orthod Dentofacial Orthop. 2015 Sep; 148(3).
- Wilcko M. accelerated osteogenic orthodontics technique: a 1- stage surgically facilitated rapid orthodontic technique with alveolar augmentation. J oral maxillofac surg.. 2009; 67(10).
- Yamasaki K SYISTYSYFT. Clinical application of prostaglandin E1 (PGE1) upon orthodontic tooth movement. American Journal of Orthodontics and Dentofacial Orthopedics. 1984; 85.
- Pavlin D ZRGHJ. Temporal pattern of stimulation of osteoblast-associated genes during mechanically-induced osteogenesis in vivo: Early responses of osteocalcin and type I collagen. Connective Tissue Research. 2001; 42.
- Pavlin D MMZRGEGHJ. Orthodontically stressed periodontium of transgenic mouse as a model for studying mechanically induced gene regulation in bone: The effect on the number of osteoblasts. Clinical Orthododontics and Research. 2000; 3.
- 20. Rubin C TSMRMEMKLWaQY. Quantity and quality of trabecular bone in the femur are enhanced by a strongly anabolic, noninvasive mechanical intervention. J Bone and Mineral Research. 2002; 17(2).
- Rubin J RCJC. Molecular pathways mediating mechanical signaling in bone.. Gene. 2006; 367.
- Gluhak-Heinrich J YLBLFJMMHSPD. Mechanical loading stimulates dentin matrix protein 1 (DMP1) in osteocytes in vivo. Journal of Bone and Mineral Research. 2003; 18.
- Andrade MSR. Ortodoncia celerada periodontalmente: fundamentos biológicos técnicas quirúrgicas. Revista mexicana de peridiodontología. 2011 abril; 2(1).
- Kawasaki K SN. Effects of low-energy laser irradiation on bone remodeling during experimental tooth movement in rats. Lasers in Surgery and Medicine. 2000; 26.
- Stark TM SP. Effect of pulsed electromagnetic fields on orthodontic tooth movement. American Journal of Orthodontics and Dentofacial Orthopedics. 1987;(91).
- Takano-Yamamoto T KMYT. Effect of age on the rate of tooth movement in combination with local use of 1,25(OH)2D3 and mechanicalforce in the rat. Journal of Dental Research. 1992; 71.
- Motohashi T NMKK. Biomechanical efffects of orthodontic treatment by using anchorage device combined with corticotomy. Journal of Cranio-Maxillofacial Surgery.. 2006; 34(1).
- Vercellotti TP. Orthodontic microsurgery: a new surgically guided technique for dental movement. Int J periodontics Restorative Dent. 2007; 27.
- Köle H. Surgical operations of the alveolar ridge to correct occlusal abnormalities. Oral Surg Oral Med Oral Pathol. 1959; 12(3).
- Frost H. The regional acceleratory phenomenom: a review. Henry Ford Hosp Med J. 1983; 31(1).
- Kanno T MMFYKSAN. Corticotomy and compression osteogenesis in the posterior maxilla for treating severe anterior open bite. Int J Oral Maxillofacial Surg. 2007;(4).
- Oliveira D OBAHGSMP. Selective alveolar corticotomy to intrude overerupted molars. Am J Orthod Dentofacial Orthop. 2008; 133.
- 33. Rubin C JSQY. Low-level mechanical signals and their potential as a non-pharmacological intervention for osteoporosis. Age and Ageing. 2006; 35(S2).
- Pavlin D GHJ. Effect of mechanical loading on periodontal cells. Critical Reviews in Oral Biology and Medicine. 2001; 12.

Reconocimiento-NoComercial-CompartirIgual
CC BY-NC-SA
Esta licencia permite a otros entremezclar, ajustar y construir a partir de su obra con fines no comerciales, siempre y cuando le reconozcan la autorÍa y sus nuevas creaciones estÉn bajo una licencia con los mismos tÉrminos.
