RESUMEN
La mordida abierta anterior es una maloclusión en que uno o más dientes no alcanzan el plano oclusal y no se establece contacto con sus antagonistas. Su tratamiento es difícil y existe controversia en la necesidad de un abordaje quirúrgico. El presente caso relata el manejo de un paciente femenino de 61 años de edad, atendido en la clínica del Instituto Mexicano de Ortodoncia, que acudió por “separación de sus dientes”. La evaluación clínica y radiográfica presentó una clase I esquelética, biprotrusiva, con overbite de -30% con sonrisa baja y no consonante, deglución atípica como factor etiológico que permitió el diagnóstico de mordida abierta anterior. El tratamiento consistió en la colocación de brackets prescripción Roth slot .022 con tubos hasta terceros molares superiores e inferiores, colocando brackets más hacia gingival con respecto al centro de la corona anatómica de ambas arcadas para lograr la extrusión y cierre de la mordida abierta y arco de sonrisa; en centrales a 1.5mm, laterales a 1mm y caninos a 0.5mm. Fue fundamental el uso de topes oclusales posteriores y también de elásticos anteriores cortos y ligeros desde el primer día del tratamiento. Se consiguió la corrección de la posición de los dientes en un tiempo de 18 meses, que además se indujo un cambio en el patrón de deglución. Mediante el plan de tratamiento propuesto se demostró que se puede dar estabilidad a la oclusión y que no todo paciente con mordida abierta es candidato a tratamiento quirúrgico para la corrección de esta maloclusión.
Palabras clave: Mordida abierta; maloclusión; deglución, adulto; manejo de caso.
ABSTRACT
The previous open bite is a malocclusion in which one or more teeth do not get the occlusal plane and no contact is made with their antagonists. Its treatment is difficult and there is controversy in the need for a surgical approach. The present case relates to the management of a 61-year-old female patient, treated at the clinic of the Mexican Institute of Orthodontics, who came for "separation of her teeth." The clinical and radiographic evaluation presented a skeletal class I, biprotrusive, with overbite of -30% with low and non-consonant smile, atypical swallowing as an etiological factor that allowed the diagnosis of anterior open bite. The treatment consisted of the placement of Roth slot .022 prescription brackets with tubes up to upper and lower third molars, placing more gingival braces with respect to the center of the anatomical crown of both arches to achieve extrusion and closure of the open bite and arch of smile; in centrals at 1.5mm, laterals at 1mm and canines at 0.5mm. The use of posterior occlusal bumpers and also of short and light anterior elastics from the first day of treatment was essential. Correction of the position of the teeth was achieved in a period of 18 months, which also induced a change in the swallowing pattern. Through the proposed treatment plan it was shown that occlusion stability can be given and that not every patient with an open bite is a candidate for surgical treatment for the correction of this malocclusion.
Keywords: Open bite; malocclusion; swallowing, adult; case management.
RESUMO
A mordida aberta anterior é uma má oclusão na qual um ou mais dentes não atingem o plano oclusal e não é feito contato com seus antagonistas. Seu tratamento é difícil e há controvérsia na necessidade de uma abordagem cirúrgica. O presente caso refere-se ao tratamento de uma paciente de 61 anos de idade, atendida na clínica do Instituto Mexicano de Ortodontia, que veio pela "separação dos seus dentes". A avaliação clínica e radiográfica apresentou classe esquelética biprotrusiva I, com sobremordida de -30% com sorriso baixo e não consoante, deglutição atípica como fator etiológico que permitiu o diagnóstico de mordida aberta anterior. O tratamento consistiu na colocação de suportes de prescrição Roth .022 com tubos até os terceiros molares superiores e inferiores, colocando os suportes mais voltados para a gengiva em relação ao centro da coroa anatômica de ambos os arcos para obter extrusão e fechamento da mordida e arco aberto de sorriso; nas centrais a 1,5 mm, laterais a 1 mm e caninos a 0,5 mm. O uso de topes oclusais posteriores e também de elásticos anteriores curtos e leves desde o primeiro dia de tratamento foi essencial. A correção da posição dos dentes foi realizada em um período de 18 meses, o que também induziu uma alteração no padrão da deglutição. Através do plano de tratamento proposto, demonstrou-se que a estabilidade da oclusão pode ser dada e que nem todo paciente com mordida aberta é candidato ao tratamento cirúrgico para correção dessa má oclusão.
Palavras-chave: Mordida Aberta; Má Oclusão; Deglutição Adulta; Redlato de Caso.
INTRODUCTION
The anterior open bite is defined as a malocclusion characterized by the deviation in the vertical relationship of the maxilla and the mandible of the anterior sector, identified by a lack of contact between opposite segments1. In this case, one or more teeth do not reach the occlusal plane and no contact is made with their antagonists. They are mainly caused by an over eruption of the upper posterior teeth, a vertical overgrowth of the posterior dentoalveolar complex or a swallowing with lingual protrusion. It is seen in individuals of any age with displaced incisors, in which it appears as an adaptation to the space between the teeth1-3.
This malocclusion is developed by the interaction of several etiological factors: variations in dental eruption and alveolar growth, disproportion in muscle growth or even an aberrant neuromuscular function related to lingual dysfunctions, oral habits or both. That is, the presence of a hyperdivergent pattern, plus an abnormal lingual position (frequently associated with airway problems) or digital sucking habits, are risk factors for its development4,5.
Until now it has not been possible to determine the exact role of inheritance as an etiological factor of this malocclusion. It has been possible to establish a high heritability in the craniofacial dimensions and relatively low in the variations of the dental arches, but the impact that it may have on the etiology of the bad occlusions that present skeletal and dental components remains unknown6-7.
This malocclusion causes discomfort to the patient given its functional, masticatory, phonetic and aesthetic ineffectiveness; It is a difficult-to-treat dentomaxillary deformity, recurrences are frequent and a comprehensive approach that encompasses functional and aesthetic aspects is required8-10.
The purpose of the present case is to analyze the treatment by means of orthodontic appliances of an adult patient with atypical swallowing who has an anterior open bite.
Case report
A 61-year-old female patient, who goes to the Mexican Institute of Orthodontics to be treated "for the separation of my teeth" without a history of any previous orthodontic treatment.
At the extraoral examination, an oval, brachifacial face, chin slightly deviated to the right and an enlarged lower third were observed. The smile analysis showed 40% of the clinical crown and a low, non-consonant and complex smile, the upper and lower midlines centered and coinciding with the facial midline. (Fig 1.)

FigurE 1. Extraoral analysis, profile and smile analysis.
In the intraoral analysis, the upper and lower midline centered, anterior open bite, adequate labial frenulum insertion was observed. Bilateral molar class I and bilateral Canine II class, 0.5mm Spee curve and gingival recessions in dental organs 33 and 43. The upper and lower U-shaped arch, diastemas, presence of third molars and crowns in dental organs 16 and 26 (Fig. 2)

Figure 2. Intraoral analysis.
In the highlight analysis, an overjet of 2mm and an overbite of -3mm (11 to 41 as a reference) were observed. (Fig. 3)

Figure 3. Highlighting photograph that allows to observe a negative overbite.
In the panoramic radiography an adequate root length and good condition of the periodontal ligament could be observed. On the lateral skull x-ray, a skeletal, biprotusive Class I, with anterior open bite, vertical growth is observed by Rickets. ( Fig. 4)
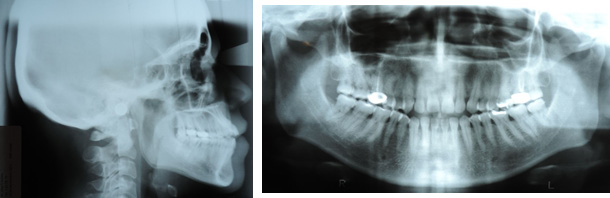
Figure 4. Panoramic and lateral x-ray of initial skull.
With a diagnosis of anterior open bite associated with atypical swallowing; He considered avoiding the surgical approach; The objectives of the orthodontic treatment plan were: maintain lower midline, shape dental arches, maintain Bilateral Molar Class I and obtain bilateral Canine I class. Improve profile, get bow smile and improve overjet and overbite.
“Full bonding” of Roth slot .022 prescription brackets was performed up to upper and lower third molars, placing brackets in centrals at 1.5 mm, laterals at 1 mm and canines at .5 mm more towards gingival with respect to the center of the anatomical crown of both arches to achieve extrusion and closure of the open bite and smile arch. The use of posterior occlusal stops and also of short and light anterior elastics (3/16 of 2.5 oz) from the first day of treatment was essential. (Fig. 5)

Figure 5. Use of occlusal stops and short and light elastics, which were essential to achieve the treatment objectives..
Results
Through the proposed treatment plan, the objective that was planned in 18 months could be fulfilled, observing that not every patient with an open bite is a candidate for surgical treatment and it was demonstrated that an orthodontic treatment can be achieved as a successful alternative. (Fig. 7 and 8)

Figure 7. Final results
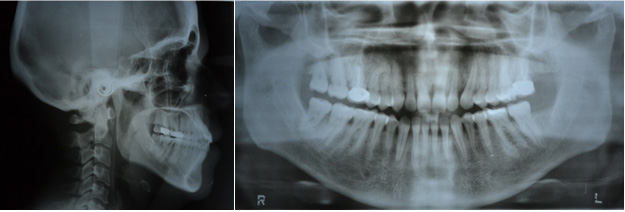
Figure 8. X-rays of final results.
Discussion
The etiology of the anterior open bite is multifactorial and includes unfavorable growth patterns. It can affect speech, swallowing, chewing and aesthetics, thus creating inadequate conditions to lead a normal social life11-13. Authors such as Zhou, Tavares and Atac, agree that patients with anterior open bite are affected in society due to low self-esteem, decreased levels of confidence and associated physiological problems14-16.
For Bennet, due to the growth potential and the patient's collaboration, the treatment of open bites, especially those associated with habits in hyperdivergent patients, should be started at an early age17-18.
Several treatment options are presented in the literature, with the aim of inhibiting the mechanical factors that maintain the anterior open bite and / or limit the excessive vertical growth of facial skeletal components. Garret 19 mentions that the adequate control of habits at an early age is very helpful, coinciding with the aforementioned by Bennet 18. However, he also mentions that when a patient reaches adulthood without any previous preventive or interceptive treatment , the management of treatment from the area of orthodontics or orthognathic surgery should be focused as required18-19.
Many therapies have been aimed at increasing the stability of the results obtained in patients with open bite, authors such as Shapiro 20 recommend that the habit of tongue wait at least two years before withdrawing the therapy used to obtain a good function and prevent recurrence20-21.
The correction of the open bite made through fixed orthodontics has been reported successfully. And the post-treatment records show favorable dentoalveolar changes with this type of therapy, as Alexander 21 reports in his studies, which have shown that only 35% of cases show significant recurrence of long-term open bite. According to López22, it is very important to note that the stability of the results obtained and the control of the factors that caused the malocclusion must be maintained, since it must be borne in mind that in the cases of patients with open bite the stability is still not predictable21-22.
Finally, it is necessary to know the orthognathic principles and limits in the orthodontic movement, as well as a correct myofunctional management, especially in the presence of bad oral habits such as atypical swallowing.
Conclusions
Atypical swallowing with dental protrusion generates displacement of the incisors due to the incorrect position of the tongue. Therefore, it follows that correcting the position of the teeth should induce a change in the swallowing pattern, as is usually the case. It was shown that the treatment applied do not need surgery to correct open bite, and can provide stability to occlusion, other factors to improve the aesthetic and functional patient.
Bibliografía
- Proffit W, Fields H, Sarver D. Ortodoncia Contemporánea 5ta. Edición, España, Elsevier. 2014.
- Moreno Sinovas E, Halabi Díaz T, Alió Sanz JJ. Tratamiento temprano vs tratamiento tardío. ¿Cuándo actuar? Parte I. Clase II y Mordida Abierta. Ortodoncia Clínica. 2009; 12(1):21-33.
- Oliveira AC, Almeida Pordeush I, Silva Torres C, Torres M. Feeding and nonnutritive sucking habits and prevalence of open bite and crossbite in children/adolescent with Down Syndrome. Angle Ortthodontist. 2010;80(4): 748-52
- Ramírez Mendoza J, Bulnes López RM, Guzmán León R, Torres López JE, Priego Álvarez HR. Características y alteraciones de la oclusión en la dentición primaria en preescolares de 3 a 6 años en Tabasco, México. Odontol Pediatr. 2011; 10(1): 6-12.
- Thilander B, Peña L y colaboradores. Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogotá, Colombia. An epidemiological study related to different stages of dental development. European J of Orthod. 2011; 23: 153-67.
- Cozza P, Baccetti T, Franchi L, Toffol L, McNamara JJr. Mandibular Changes produced by Functional appliances in Class II Malocclusion: A sistematic Review. AJO. 2008; (5): 8.
- Thilander B, Peña L y colaboradores. Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogotá, Colombia. An epidemiological study related to different stages of dental development. European J of Orthod. 2011; 23: 153-67.
- Proffit WR, Fields HN, Maray LL. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHAMES III Survey. Int J Osthognath Surg. 2003; 13 (2):97-106.
- Cangialosi TJ. Skeletal morphologic features of anterior open bite. Am J Orthod. 2008; 5:28-36.
- Proffit WR. The timing of early treatment: an overview. Am J Orthod Dentofac Orthop. 2001; 129(4):47-9.
- Ngan P, Fields HW. Open bite: a review of etiology and management. PediatrDent. 1997 Mar-Apr;19(2):91-8.
- Cozza P, Baccetti T, Franchi L, Mucedero M, Polimeni A. Sucking habits and facial hyperdivergency as risk factors for anterior open bite in the mixed dentition. Am J Orthod Dentofacial Orthop. 2005 Oct;128(4):517-9.
- Xin N, Tao W, Ashwin D, Jinlin S. Establishment of integral biomechanical
- Zhou Y, Li Z, Wang X, Zou B, Zhou Y. Progressive changes in patients with skeletal Class III malocclusion treated by 2-jaw surgery with minimal and conventional presurgical orthodontics: a comparative study. Am J Orthod Dentofacial Orthop. 2016 Feb;149(2):244-52.
- Tavares CAE, Allgayer S, Calvete ED, Polido WD. Orthodontic treatment for a patient with advanced periodontal disease: 11-year follow-up. Am J Orthod Dentofacial Orthop. 2013 Sept;144(3):455-65.
- Ataç M, Asvaroğlu K, Yücel E. Prospective evaluation of quality of life in orthognathic surgery patients. Int J Oral Maxillofac Surg. 2015;44(1 Suppl 1):e31.
- Marwat HJ, Amin B, Khan A. Frequency of anterior open bite patients reporting to AFID, RAWALPINDI. Pakistan Oral & Dental Journal. 2009; 281(1): 71-4.
- Bennet Greg and col Efficacy of Open-Bite Treatment with the Thera-spoon. JCO 1999 33:5, 283-285.
- Garrett J, Araujo E, Baker C. Open-bite treatment with vertical control and tongue reeducation. Am J Orthod Dentofacial Orthop. 2016 Feb;149(2):269-76.
- Shapiro Peter. Stability of open bite treatment. Am J Orthod Dentofacial Orthop 2002;121:566-8.
- Alexander Charles Open bite, dental alveolar protrusion, Class I malocclusion: A successful treatment result Am J Orthod Dentofacial Orthop 1999;116:494-500
- Lopez-Gavito G, Wallen TR, Little RM, Joondeph DR. Anterior open bite malocclusions: a longitudinal 10-year postretention evaluation of orthodontically treated patients. Am J Orthod 1985;87:175-86.
 |
|
| |
| |
| |

Reconocimiento-NoComercial-CompartirIgual
CC BY-NC-SA
Esta licencia permite a otros entremezclar, ajustar y construir a partir de su obra con fines no comerciales, siempre y cuando le reconozcan la autorÍa y sus nuevas creaciones estÉn bajo una licencia con los mismos tÉrminos.