RESUMEN
En ortodoncia es de relevante importancia crear una oclusión estéticamente agradable y funcional, además de lograr y preservar el óptimo atractivo facial; es mandatorio realizar un examen facial minucioso porque el equilibrio y la armonía de las diferentes partes de la cara está determinada por los tejidos du-ros y blandos. El objetivo del presente artículo es exponer la importancia de un diagnóstico integral al momento de la planificación del tratamiento. El presente caso, relata el manejo ortodóntico con filosofía Roth de una paciente de 13 años de edad, raza latina, diagnosticada con relación esquelética clase II, proinclinación excesiva de los incisivos en ambos arcos, perfil convexo e hi-pertonicidad del mentón. El plan de tratamiento se planificó para corregir la y la clase II esquelética mediante extracciones de los 4 primeros premolares. Como resultado se eliminó la hipertonicidad muscular, obteniendo una competencia labial adecuada y se mejoró el perfil facial en un tiempo de 18 meses. El mane-jo de este caso resulta exitoso gracias a un diagnóstico correcto y la planifica-ción del caso, permite demostrar que no solo son objetivos ortodónticos las es-tructuras óseas y dentales, sino también aquellos que ayudan a mejorar el per-fil facial del paciente. Fue necesario evaluar la relación de los labios y la barbi-lla ya que estos pueden alterarse con el tratamiento de ortodoncia.
Palabras clave: Hipertonía Muscular; Mal Oclusión; Manifestaciones Neuromusculares; malo-clusión de Angle Clase II.
ABSTRACT
In orthodontics It’s of relevant importance to create an aesthetically pleasing and functional occlusion, in addition to achieving and preserving the optimal facial attractiveness; It is mandatory to perform a thorough facial exam because the balance and harmony of the different parts of the face is determined by soft and soft tissues. The objective of this article is to expose the importance of a comprehensive diagnosis at the time of treatment planning. The present case relates the orthodontic management with Roth philosophy of a 13-year-old Latina patient, diagnosed with a class II skeletal relationship, excessive incision of the incisors in both arches, convex profile and chin-hypertonicity. The treatment plan was planned to correct the skeletal class II by extractions of the first 4 premolars. As a result, muscular hypertonicity was eliminated, obtaining adequate lip competence and the facial profile was improved in a period of 18 months. The management of this case is successful thanks to a correct diagnosis and the planning of the case, allows to demonstrate that not only are the bone and dental structures orthodontic objectives, but also those that help improve the patient's facial profile. It was necessary to evaluate the relationship of the lips and chin since these can be altered with orthodontic treatment.
Keywords: Muscular Hypertonia; Bad Occlusion; Neuromuscular Manifestations; Angle Class II malocclusion.
RESUMO
A mordida aberta anterior é uma má oclusão na qual um ou mais dentes não atingem o plano oclusal e não é feito contato com seus antagonistas. Seu tratamento é difícil e há controvérsia na necessidade de uma abordagem cirúrgica. O presente caso refere-se ao tratamento de uma paciente de 61 anos de idade, atendida na clínica do Instituto Mexicano de Ortodontia, que veio pela "separação dos seus dentes". A avaliação clínica e radiográfica apresentou classe esquelética biprotrusiva I, com sobremordida de -30% com sorriso baixo e não consoante, deglutição atípica como fator etiológico que permitiu o diagnóstico de mordida aberta anterior. O tratamento consistiu na colocação de suportes de prescrição Roth .022 com tubos até os terceiros molares superiores e inferiores, colocando os suportes mais voltados para a gengiva em relação ao centro da coroa anatômica de ambos os arcos para obter extrusão e fechamento da mordida e arco aberto de sorriso; nas centrais a 1,5 mm, laterais a 1 mm e caninos a 0,5 mm. O uso de topes oclusais posteriores e também de elásticos anteriores curtos e leves desde o primeiro dia de tratamento foi essencial. A correção da posição dos dentes foi realizada em um período de 18 meses, o que também induziu uma alteração no padrão da deglutição. Através do plano de tratamento proposto, demonstrou-se que a estabilidade da oclusão pode ser dada e que nem todo paciente com mordida aberta é candidato ao tratamento cirúrgico para correção dessa má oclusão.
Palavras-chave: Mordida Aberta; Má Oclusão; Deglutição Adulta; Redlato de Caso.
INTRODUCTION
It is considered that the main objective of orthodontics is to create an aesthetically pleasing and functional occlusion, as well as to achieve and preserve the optimal facial attractiveness, therefore, it is mandatory for an orthodontist to perform a thorough facial exam because balance and harmony of the different parts of the face is determined by hard and soft tissues.1-2
Clinical observation of the patient is essential to detect relevant situations that suggest certain considerations that complement the therapeutic planning of a clinical case.1 Almost two decades ago, Arnett and Berg-man (2004) introduced the "cephalometric analysis of tissues. soft, "since then, treatment based on soft tissue measurements has been receiving more attention.3-4
The height and projection of the chin has an important role in facial harmony.3-4 Chin hypertonicity suggests a labial incompetence, since it affects facial aesthetics, taking into account that currently it has increased its demand in the number of patients, this being a re-lifting factor to complete an orthognathic and orthodontic treatment.5-6
There are more than twenty muscles in the human face. Particularly in the area of the lips and cheeks; Many muscles converge or intermingle. their functional harmony and balance is very important in the growth and development of the craniofacial region. 2 Lip incompetence is caused by the orbicularis muscle of the lips, which is a concentric muscle around the mouth. The elevation and protrusion of the central aspect of the lower lip is governed by the chin muscles.7-8
The tissues around the teeth, the tongue and on the other hand the cheeks and lips, must maintain a balance. When this balance is lost, some malocclusion can occur due to the malfunction of the peri-oral musculature, so it is common to find protrusion of the incisors, causing a greater displacement of the lips to achieve closure, presenting the hypertonicity of Chin muscles.9-10
For this reason, this article reports the importance of focusing integrally on the clinical findings that can be found in a patient, both in hard and soft tissues; since, there are structures that can guide a better result, both aesthetic and functional, if they are correctly diagnosed and included in each patient's treatment plan.
Case report
A 13-year-old female patient visits the clinic of the Mexican Institute of Orthodontics (IMO), whose reason for consultation was "I have crooked teeth." she had no history of previous orthopedic or orthodontic treatment. In the extraoral analysis, the lower third slightly increased with hypertonicity of the chin muscles, which suggested a labial incompetence. Convex profile and labial biprotrusion were observed (Figure 1). Through the smile analysis, it was possible to see that the upper and lower dental midlines are coincident (Figure 2).

Figure 1. Front and profile photography. A and B allow observing the hypertonicity of the chin.

Figure 2. Análisis extraoral: fotografía de sonrisa: líneas medias dentales superior e inferior son coincidentes.
In the intraoral analysis, she showed periodontium with normal characteristics, coincident upper and lower and lower dental lines, moderate anterior crowding, gyroversion of the dental organ 21 and dental organ 23 in infraocclusion. The bilateral molar class I, canine class II is distinguished by bilateral projection, proinclination of the right upper central and lateral incisors. (Figure 3)

Figure 3. The bilateral molar class I is distinguished, canine class II by bilateral projection, proinclination of the right upper central and lateral incisors.
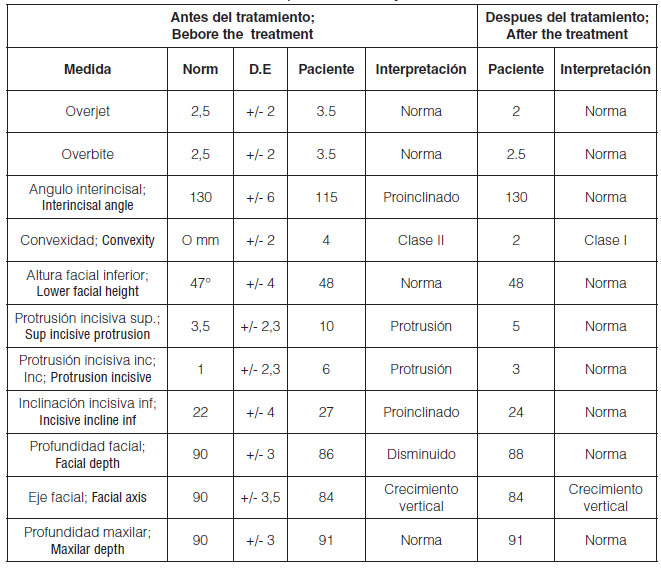
In the panoramic radiography an adequate root length and presence of third molars were observed. Lateral x-ray of the skull in conjunction with Ricketts cephalometric analysis suggested a skeletal class II malocclusion, with an increase in the lower third of the face, incision of the incisors and a convex profile due to a slight rotation of the jaw (Figure 4 -chart 1).

Figure 4. A: Panoramic x-ray and B: skull lateral.
Based on the clinical evaluation and the cephalometric traces, a Class II skeletal relationship was diagnosed, by retrognathism, with posterior rotation of the jaw, due to a decrease in the occlusion plane. Facial biotype Severe dollar. Dentally, bilateral Molar Class I and bilateral Canine Class II. Proinclination of the incisors in both arches.
The objectives of the treatment were to maintain the molar Class I dental relationship and correct the canine Class II, obtain a functional occlusion, eliminate the habit of anterior interposition of the tongue during swallowing, correct the hypertonicity of the chin muscles and improve the facial profile.
The treatment was carried out by extractions of the first four premolars (dental organ 14,24,34 and 44), a moderate anchorage was placed with a transpalatinal arch and a lingual arch. Roth slot 0.022 ”“ full bonding ”prescription brackets were cemented. Space closure was performed by displacement through surgical posts, using intermaxillary elastics. And finally for containment, superior circumferential retainer and lower fixed retention were placed.
After 18 months, the planned objectives were gotten, the hypertonicity of the chin muscles was reduced, which allowed an adequate labial competence, the bad oral habit developed (lingual interposition) was controlled. The occlusal phase and facial profile aesthetics were improved by eliminating lip bi-protrusion. (Fig. 5) (Fig. 6)

Figure 5. Final extraoral photographs: the reduction of chin hypertonicity is observed.

Figure 6. Final intraoral photographs: occlusal function, Class I molar and bilateral canine, shaped arches and coincident central midlines.
Table 1. Comparison of the initial and final cephalometric analysis.
Discussion
he proposed treatment was developed satisfactorily thanks to the fact that dental and muscular conditions were considered from the beginning. When maclusions are resolved with orthodontics, there may be some patients who are not satisfied with the results. Therefore, in this case, the decisions for the execution of a treatment plan were based on the list of problems that arose, in addition to considering the patient's wishes with the expectation of the result.11-12-13
Min-Ho et al. (2010), described the importance in chin aesthetics and concluded that this is an indispensable prominent component of the aesthetic profile line. Likewise, Auger and Turley (1999), have already identified the chin as a fundamental characteristic in the craniofacial complex, since its morphology has an impact on the diagnosis and treatment planning in orthodontic patients; They mentioned that the chin serves as an anatomic guide and reference for aesthetics in the lower third of the face; According to these concepts, the chin analysis was a key factor in the diagnosis and one of the fundamental objectives of the proposed treatment.6-14
Arnett and Bergman (1993), published an article in which they consider relevant soft tissue analysis to maintain facial aesthetics and harmony, as well as part of a better treatment plan for ortho-donation patients . This criterion was applied in our clinical case, since there are facial features in the analysis of the patient that should be studied further; As stated in this article, the hypertonia of the chin muscles that results in a labial incompetence.15-16-17
On the other hand, Bader (1991), explained that dentoalveolar protrusion causes changes in the facial profile, these are reflected in factors such as labial incompetence, chin hypertonicity and gingival dysplasia; He mentioned that once the position of the incisors is corrected, relaxation of the chin muscles is observed.18-19-20
Other authors argue that, during clinical diagnosis and treatment planning, emphasis is placed on the examination of the chin, hard, soft tissue and its relation to the position of the incisors. In the case presented, the analyzes showed that the chin hypertonicity to produce the forced closure of the lips was probably due to the position of the upper and lower incisors, since it is presented as a physical barrier to achieve a normal labial closure. , as already mentioned by authors such as Guttafsson.20-21-22
Regardless of the characteristics inherent to each type of face, beauty exists if there is symmetry, balance and proportion. The teeth have an indirect influence on the aesthetics of the facial profile, depending on the anteroposterior position of these the support for the lips and vermilion can be affected. In this case, we have shown that a successful outcome in a patient after orthodontic treatment could depend in part on a correct position and function of their soft tissues.21-22-23
Conclusions
The handling of this case, allows to demonstrate that a correct muscular function is a key factor to achieve the stability of a treatment; Not only are bone and dental structures orthodontic, but also those that help improve the patient's facial profile. It was necessary to evaluate the relationship of the lips and chin since these can be altered with orthodontic treatment.
Bibliografía
- Sercan Alkyacin et al. Smile esthetics: Evaluation of long-term changes in the transverse dimensión. Korean J Orthod 2017;47(2):100-107
- Shikha Singh, Sonali Deshmukh. Mean values of Arnett's soft tissue anal-ysis in Maratha ethnic (Indian) population — A cephalometric study. J Int Soc Prev Community Dent. 2016 Jul-Aug; 6(4): 327
- Arnett, W., & Gunson, M. (2004). Facial planning for orthodontists and oral surgeons. American Journal of Orthodontics and Dentofacial Orthopedics, 290-295.
- Bergman, R. W.-F. (2014). Longitudinal study of cephalometric soft tissue profile traits between the ages of 6 and 18 years. Angle Orthodontics, 48-55.
- Sergio Paduano, Roberto Rongo, , Rosaria Bucci, Giuseppe Carvelli and Iacopo Cioffi. Impact of functional orthodontic treatment on facial attractive-ness of children with Class II division 1 malocclusion. European Journal of Orthodontics, 2019, 1–7.
- Min-Ho Junga ; Won-Sik Yangb ; Dong-Seok Nahmb. Maximum Closing Force of Mentolabial Muscles and Type of Malocclusion. Angle Orthod 2010;80:72–79.
- Nisa Guel Amuk, and co. Effects of Different Head Positioning Methods on Facial Soft Tissue Analysis Using Stereophotogrammetry. 2019 American Association of Oral and Maxillofacial Surgeons J Oral Maxillofac Surg 77:1277.e1-1277.e10, 2019
- Fernandez VJM. A study of the development of the orbicularis oris muscle. Plast Reconstr Surg. 1975;55: 205–213
- Nomura M, Motegi E, Hatch JP, et al. Esthetic preferences of European American, Hispanic American, Japanese and African judges for soft-tissue profiles. Am J Orthod Dentofacial Orthop 2009;135:S87–95.
- Rashna Hoshang Sukhiaa, Hoshang Rumi Sukhiab, Syed Iqbal Azamc, Mubassar Fidad, Munizeh Khane. Chin Position: to treat or not to treat. In-ternational Orthodontics 2017 ; X : 1-9
- Spalding P. Treatment of Class II malocclusion. In: Bishara SE, ed. Text-book of Orthodontics. Philadelphia, Pa: WB Saunders; 2001:324–374.
- Jin-Hyoung Cho,a Eun-Jung Kim,b Byeong-Chae Kim,c Ki-Hyun Cho,d Ki-Heon Lee,e and Hyeon-Shik Hwang Correlations of frontal lip-line canting with craniofacial morphology and muscular activity. Am J Orthod Dentofa-cial Orthop 2007;132:278.e7-278.e14
- Sarver DM, Ackerman MB. Dynamic smile visualization and quantification: part 1. Evolution of the concept and dynamic records for smile capture. Am J Orthod Dentofacial Orthop 2003;124:4-12.
- Sarver DM, Ackerman MB. Dynamic smile visualization and quantification: part 2. Smile analysis and treatment strategies. Am J Orthod Dentofacial Or-thop 2003;124:116-27.
- Auger TA, Turley PK. The female soft tissue profile as presented in fashion magazines during the 1900s: a photographic analysis. Int J Adult Orthod Orthognath Surg 1999;14:7-18.
- Arnett, W., & Bergman, R. Facial keys to orthodontic diagnosis and treat-ment planning. Part I. American Journal of Orthodontics and Dentofacial Orthopedics, 1993. 299-312.
- Matta, C., & Sagawa, J. Comparación entre la zona facial media y el tercio facial inferior en estudiantes de 19 a 25 años de edad de la FacuItad de Estomatología de la UPCH. Revista Estomatológica Herediana, 13 (2-3), 23-26, 2003.
- Bader HI. Soft-tissue considerations in esthetic dentistry. Compendium 1991;12:534, 536-8, 540-2.
- Spalj S, Slaj M, Varga S, Strujic M, Slaj M. Perception of orthodontic treat-ment need in children and adolescents. Eur J Orthod 2010;32:387–94.
- Craig R. Scott,a Mithran S. Goonewardene,b and Kevin Murrayc Influence of lips on the perception of malocclusion. Am J Orthod Dentofacial Orthop 2006;130: 152-62
- Sukhia RH, Khan M, Fida M, Shaikh A, Azam SI. Esthetic preferences for facial soft tissue profiles. Int J Orthod Milwaukee 2011;22:17–23.M.
- Guttafsson and J. Ahlgren. Mentalis and Orbicularis Oris Activity in Cbiktren With Incompetent Lips: An Electromyographic and Cephalometric Study. Acta Oaontol. Soanrl. 33:1975
- Sarver DM, Ackerman JL. Orthodontics about face: the re-emergence of the esthetic paradigm. Am J Orthod Dentofacial Orthop 2000;117:575–6.

Reconocimiento-NoComercial-CompartirIgual
CC BY-NC-SA
Esta licencia permite a otros entremezclar, ajustar y construir a partir de su obra con fines no comerciales, siempre y cuando le reconozcan la autorÍa y sus nuevas creaciones estÉn bajo una licencia con los mismos tÉrminos.
